THE BLUEPRINT: How Health Regulatory Bodies Can Move From Cultural Safety Commitment to Structural Transformation
By Jayde Fuller - Indigenous Regulatory Practice
Suggested citation
Fuller, J. (2026, June 8). The Blueprint: How health regulatory bodies can move from cultural safety commitment to structural transformation. Indigenous Regulatory Practice. https://doi.org/10.5281/zenodo.20586944
The Gap Nobody Names
Most health regulatory bodies have committed to cultural safety. Almost none have achieved it. This article is about why - and what crossing that threshold actually requires. Spoiler: it is not more culturally themed morning teas. Nor is it pulling Indigenous practitioners away from caring for our people to brief non-Indigenous staff on days of cultural significance.
Though written for regulators, this applies to any health institution that holds power over Indigenous Peoples.
The gap between commitment and structural transformation has two threshold conditions. They must happen in this order:
rescinding white and institutional power (power over Indigenous Peoples); and
respecting and supporting the self-determination, leadership, knowledges and governance of Indigenous Peoples.
First Nations and Indigenous Peoples know this gap intimately. We feel it in our bodies, minds and spirits. It hits us when non-Indigenous staff, leaders or Board members minimise us. They minimise our ways of being, our ideas and our experiences, or deem them invalid.
This impact shows up as:
racism (the impact on us matters more than your label or your intentions);
reinforcement of white supremacy culture and the colonial project;
mis-deployment of Indigenous staff;
deterioration of our psychosocial wellbeing [1];
disengagement, silencing and self-censorship;
resignation from the workplace;
tokenistic representation mistaken for governance;
erosion of trust with Aboriginal and Torres Strait Islander / First Nations communities.
What Transformation Is Not
Many interventions in health regulation feel like progress. But they do not change the structure that should prioritise cultural safety. On the surface, some look promising to insiders and stakeholders. They read as markers of transformation. Yet they fall short of both threshold conditions above.
Here are some typical examples from health regulation.
Cultural safety training
It seems reasonable to believe that training produces a culturally safe workplace. Educate the practitioners, the non-Indigenous staff and the Board members - and surely behaviour changes? After all, registered practitioners earn the privilege of treating our populations through rigorous education, testing and practice. Right?
Training has its place. At an individual level, it can shift awareness and build a foundation. But we must be honest about who avoids change here. The regulatory body. The institution. The system.
What this belief fails to acknowledge:
Cultural safety is a lifelong commitment, not a competency you pass or fail. A training session is not the finish line. There is no finish line.
Health regulatory bodies exist because practitioners sometimes fail their obligations. So why assume training works differently? Why assume attendance alone guarantees changed behaviour?
Training frames cultural safety as a knowledge deficit. It implies that if non-Indigenous people knew more, they would act differently. This misdiagnoses the problem. Racism in healthcare is not mainly a knowledge gap. It is a power-and-accountability gap. Training addresses the wrong variable.
Training locates the problem in individuals, not the system. That lets the institution off the hook. When someone acts unsafely after training, the story becomes “that individual failed”. It does not become “this system has no structural accountability”. The institution stays blameless.
Centuries of colonisation and white supremacist culture have shaped every institution we work within. The racist beliefs they produced are not undone in one session. Indoctrination built over lifetimes does not unravel in a morning.
Showing up gets treated as enough. Training becomes a compliance box ticked, not a practice changed. Without accountability designed by and answerable to Indigenous Peoples, patients and staff, neither threshold is met.
Training without consequence is optional in practice. Even when attendance is mandated, application is not. Nothing connects what someone learned on Tuesday to how they treat an Aboriginal patient on Wednesday. The transfer gap is structurally guaranteed.
It places the burden of proof on Indigenous Peoples. We are implicitly required to prove that harm occurred. Meanwhile the practitioner’s good intentions and attendance count as mitigating evidence. The accountability architecture is inverted.
Institutional KPIs measure the wrong things - attendance numbers and the sentiment of non-Indigenous participants. “Do you feel more culturally safe?” is not asked of Aboriginal and Torres Strait Islander Peoples. It is asked of the people whose behaviour needs to change.
Indigenous ‘advisory’ committees
I have heard this many times. “We don’t know what we don’t know. Indigenous Peoples just need to tell us what they want.” “But Jayde,” I hear you say, “isn’t that threshold condition two? Respecting Indigenous leadership?” Asking is not the same as ceding. The power to ignore what you have been told stays entirely intact.
I hate to break it to you. If you have not enacted condition one first - rescinding white and institutional power - you are reproducing ‘colonial load’.[2] Weenthunga Health Network defines it as:
the load placed knowingly and unknowingly on First Nations people by settlers and institutions. It includes biases, assumptions, expectations and entitlement held by Settlers. Settlers are often ignorant and in denial of the load’s existence. The load is highly visible to us as First Nations people. When the burden to carry the load is placed on us, it causes harm. It can lead to burnout and impact our ability to maintain our cultural responsibility.
You are essentially telling First Nations Peoples something stark. Their intellectual labour, experiences and knowledge can be extracted at any time. But you are under no obligation to act on it, because the power structure stays unchanged.
So what does the institution do with that expertise? It filters the knowledge through existing power structures. It reinterprets it to fit what it was always going to do. Then it cites it as evidence of Indigenous consultation. The knowledge gets laundered. That is the colonial mechanism operating in plain sight.
Look at the word naming the committee: ‘advisory’. This is not phoning a friend about your Friday-night outfit, advice you can take or leave. The Indigenous people on that committee need real power. They need decision-making and authorising power to effect structural change, independent of the regulatory body’s hierarchy. Without it, you will burn out those staff, Board members and practitioners - or erode their trust fast.
It also carries an unwanted cost to the institution. It signals to Indigenous communities that this body does not listen to or care about our people. Our communities are small and deeply relational. Relationships are the infrastructure through which knowledge, trust and accountability move. This is not incidental to how we operate. It is the governance mechanism itself.
Western institutions tend toward transactional relationships. So they underestimate how fast reputational damage travels through Indigenous networks. They also underestimate how hard it is to repair. That is especially true when it affects our safety, our access to care, or our ability to advocate for our communities.
Indigenous staff in roles without authority
You may have Indigenous Peoples on your payroll, appointed to improve cultural safety and access. But without real authority to enact structural change, this is window dressing. It is a photo opportunity for an employment strategy. And it is deeply disempowering for those staff.
Then there is the role design problem. These positions are often created without a clear mandate. They lack reporting lines that give genuine influence. They lack resourcing matched to the scope of change required. The disempowerment is baked into the job description before the person starts. That is not an individual failure. It is an architectural one.
An anti-racism policy where non-Indigenous HR staff decide complaint outcomes
Picture an anti-racism policy where non-Indigenous HR staff control the process and outcome of harm declared by Indigenous Peoples. That is not accountability. It is the institution investigating itself. The power to define racism, and to decide a proportionate remedy, stays with the people least positioned to judge it.
The Two Thresholds
A threshold is not a milestone. Milestones can be reported against, celebrated and filed away. A threshold is a structural shift. It is the moment the architecture of power changes irreversibly. The next board cannot undo it. Neither can the next budget cycle, nor the next executive who downgrades cultural safety.
There are two thresholds. They must happen in order.
Threshold One: The Rescinding of White and Institutional Power
This is the one nobody wants to name directly. It requires the institution to make a genuine transfer. Not a consultation. Not a partnership. Not a seat at a table it still controls. It means an actual relinquishment of decision-making authority over the lives, care and futures of Indigenous Peoples.
We have seen it happen. In 2013, the First Nations Health Authority (FNHA) became the first province-wide First Nations health authority in Canada.[3] Health Canada did not partner with FNHA. It ceded jurisdictional authority to it. The federal government transferred responsibility for the design, delivery and governance of health services to an Indigenous-led body. That body is accountable to First Nations Peoples and governed by First Nations Peoples, on First Nations terms. That is Threshold One in practice. It is not symbolic. It is architectural.
Most health regulatory bodies have not come close.
Threshold Two: Respecting and Supporting Self-Determination, Leadership, Knowledges and Governance
The second threshold is not softer than the first. But it is more specific. It requires the institution to actively support Indigenous Peoples’ authority to determine outcomes that affect them. Not to consult. Not to advise. To determine.
British Columbia is instructive here too, and not by accident. The province has built a layered architecture. The sequence in which it was built is precisely what gives it force.
Indigenous governance authority was established at the apex through FNHA. So the practitioner and organisational layers that followed had something real to answer to. In 2022, the British Columbia College of Nurses and Midwives (BCCNM) brought a new practice standard into force.[4] It made cultural safety a regulatory obligation for every nurse and midwife in the province. Not an aspiration. A condition of practice. Developed with Indigenous authority behind it, the standard creates enforceable individual accountability.
Alongside this, the Health Standards Organization developed a standalone BC Cultural Safety and Humility Standard.[5] Its structure matters as much as its content. It is not absorbed into patient safety frameworks. It is not embedded as a sub-criterion of quality care. That absorption is how cultural safety is quietly diluted elsewhere. This standard exists independently. Organisations cannot cross-reference their way out of it. They must demonstrate it on its own terms.
The result is three distinct layers of accountability working in concert. Indigenous governance authority sits at the apex, in FNHA. Practitioner-level accountability runs through the BCCNM standard. Organisational accountability runs through a standalone accreditation standard that other criteria cannot satisfy. No single layer can be gamed in isolation. An organisation cannot demonstrate cultural safety at accreditation while its practitioners stay unaccountable to the practice standard. And both layers sit where Indigenous governance authority exists and holds real power.
Critically, the standards came after the governance architecture, not before it. That sequencing is not incidental. The BCCNM and HSO standards have teeth because the FNHA exists to give them teeth. Where standards are built without that governance foundation, they tend to become documents. Organisations perform compliance with them rather than transform toward real accountability.
In Australia, the framework governing health practitioner regulation has changed by law. The Aboriginal and Torres Strait Islander National Special Issues Committees now help determine the outcome of culturally unsafe care.[6] This represents meaningful movement toward Threshold Two. Indigenous Peoples are not being asked to advise on what should happen to a practitioner who caused harm. They are making that determination. That is structurally different.
It is worth being honest about what this example also shows. Accountability mechanisms can move toward Threshold Two before Threshold One is enacted. Has institutional power genuinely been rescinded? Or can the institution still wind these mechanisms back? That is a different and still-open question.
Most regulatory bodies have enacted neither threshold. Many are nowhere near Threshold One. In most cases, the gap between what is achieved and what strategy documents claim is significant. That gap is not accidental. It is structurally produced - by the same architectures that cultural safety transformation is meant to dismantle.
What It Actually Feels Like
Are you a non-Indigenous executive, leader or board member? Then I want to be honest about what this work will ask of you. Not to frighten you. I want to stop you misreading what comes next as failure. It is, in fact, evidence that something real is happening.
You will need epistemic humility. That is not a soft ask. It means genuinely recognising that your ways of knowing, doing and being are not the only ones that exist. The frameworks through which you understand governance, accountability, evidence and leadership are one set. Not the set. One.
Indigenous knowledges have sustained peoples and communities for more than sixty thousand years. They are not primitive, not pre-scientific, not in need of translation into Western frameworks to become valid. They are complex, relational and deeply nuanced. And they do not operate through the zero-sum logic that whiteness typically defaults to.
Zero-sum logic holds that for one group to gain, another must lose. It is a scarcity framework. It treats power, authority and legitimacy as finite resources to compete over, not capacities that can be structured differently. Ibram X. Kendi traces how this logic underpins some of today’s most dangerous ideologies.[7] These include Great Replacement Theory - the belief that one group’s advancement is an existential threat to another. The same logic operates, often unnamed, in institutional resistance to Indigenous governance. The assumption is that if Indigenous peoples gain authority, white institutions must be losing something. That if Indigenous knowledges are validated, Western frameworks are diminished. That power shared is power lost.
This is a false frame. But it is a persistent one. It is embedded in the epistemological architecture of the very institutions we are asking to change.
Indigenous relational epistemologies do not begin from scarcity. Right or wrong, compliant or non-compliant, inside or outside the standard - these categories are not universal. They are design features of systems built to serve white institutional interests. And they consistently fail to account for the sophistication of Indigenous governance, knowledge and community. When you feel the pull to resist relinquishing power, ask which framework is generating that feeling. The zero-sum lens is not revealing a truth about power. It is obscuring one.
Here is the harder thing. Systems and institutions are built around white comfort. That is not an accusation. It is a structural diagnosis. So genuinely supporting cultural safety for Aboriginal and Torres Strait Islander / First Nations Peoples will require something of you. You will need to become uncomfortable. And stay there.
That discomfort has two faces. The first is internal. It is recognising where your instincts come from. Your default judgements and your sense of what is normal were shaped by institutions not designed with Indigenous peoples in mind. That is uncomfortable to sit with.
The second is interpersonal. Structural change requires you to challenge institutional norms in the room. Those norms are held by your peers - people who share your professional culture, your career context and often your race. That carries social and professional cost. It will not always be received well.
I am not telling you this so you retreat from it. I am telling you for a reason. If you wait for this work to feel comfortable before you commit, you will wait indefinitely. The discomfort is not the obstacle. The discomfort is the mechanism.
What Indigenous Leadership Actually Means
Not consultation. Not a seat at the table. Decision-making authority. Governance with real teeth.
Indigenous leadership is not a seat at the table. By now, I hope that is clear. Let me be precise about what it is.
Indigenous governance - the real kind - means decision-making authority. Not advisory authority. Not the authority to recommend, submit or be consulted. The authority to decide. That authority must come with the resources to act on decisions. On our terms - not contingent on institutional approval of how we use them.
It means leadership without conditions. Non-Indigenous institutions habitually support Indigenous leadership in principle while attaching conditions in practice. Conditions about process. About format. About which governance structures count as legitimate. Those conditions are how institutional power reasserts itself over Indigenous authority. Genuine support means withdrawing them.
It means accountability to community. Often Indigenous leaders and governance bodies are accountable mainly to the institution that funds or hosts them. That structure reproduces the colonial relationship. It positions the institution as the authority Indigenous leaders must answer to. Genuine Indigenous governance inverts that. Accountability runs to community. It runs to the Indigenous peoples whose health, safety and lives are at stake. If our practice or decisions are challenged, that challenge should come from the people we serve. Not from white institutions.
This is not a theoretical position. It is a practical one. Institutions that genuinely supported Indigenous governance have had to make real changes. They changed how they structure authority, how they resource it and how they understand their own role. They have had to move from centre to periphery. That shift is what Threshold One requires. Indigenous leadership is what becomes possible on the other side of it.
The Question for Every Health Regulatory Body
Every health regulatory body I have met can say yes to one question: “Are you committed to cultural safety?” The commitment is rarely the problem. Commitments are made at board level, written into strategic plans, announced at events and cited in annual reports.
The question that determines whether transformation is possible is different. It is not about commitment. It is about relinquishment. What are the institution, and the people who hold power within it, genuinely willing to give up? Decision-making authority. The comfort of familiar processes. The safety of institutional consensus. The assumption that Western frameworks are the right lens for evaluating Indigenous leadership.
What are you willing to relinquish?
Has that question landed somewhere real? Has it named something about where your organisation is, or where it is stuck? Then I would welcome a conversation.
Discovery Sessions with Indigenous Regulatory Practice begin here. To book one, email me at indigenousregulatorypractice@gmail.com.
References
Wilkes B, et al. - Embedding cultural safety to combat racism against Aboriginal and Torres Strait Islander peoples. Australian Journal of General Practice (RACGP); March 2026. https://www1.racgp.org.au/ajgp/2026/march/embedding-cultural-safety-to-combat-racism-against↩
Weenthunga Health Network - definition of 'colonial load'. https://weenthunga.com.au/↩
First Nations Health Authority - About the FNHA (Province of British Columbia / FNHA). https://www.fnha.ca/about↩
BC College of Nurses and Midwives - Indigenous Cultural Safety, Cultural Humility and Anti-Racism Practice Standard (effective 25 February 2022). https://www.bccnm.ca/RN/PracticeStandards/Pages/CulturalSafetyHumility.aspx↩
Health Standards Organization - British Columbia Cultural Safety and Humility Standard (HSO 75000:2022). https://healthstandards.org/standard/cultural-safety-and-humility-standard/↩
Australian Health Practitioner Regulation Agency - Aboriginal and Torres Strait Islander Health and Cultural Safety Strategy: Communiqués. https://www.ahpra.gov.au/About-Ahpra/Aboriginal-and-Torres-Strait-Islander-Health-Strategy/Communiques.aspx↩
Ibram X. Kendi - Chain of Ideas: The Origins of Our Authoritarian Age (2026). https://www.penguinrandomhouse.com/books/778233/chain-of-ideas-by-ibram-x-kendi/↩
"What-Aboutism" as Colonial Technology: A Guide for First Nations Peoples
What-aboutism deflection is not a communication failure. It is colonial technology - an automated institutional defence that activates when First Nations Peoples name specific harm and demand specific accountability. This piece argues that what-aboutism functions as a discursive mechanism with identifiable patterns, a documented history, and measurable consequences: in the 18 months following the Voice to Parliament referendum, over half of Aboriginal and Torres Strait Islander adults experienced discrimination when seeking healthcare. Discrimination is escalating - not improving - precisely as the frameworks designed to address it are being diluted.
By Jayde Fuller
Suggested Citation
Fuller, J. (2026). "What-aboutism" as colonial technology: a practical guide for First Nations People - how deflection operates as an automated defence system and how to respond from sovereignty. Indigenous Regulatory Practice. https://doi.org/10.5281/zenodo.18948592
Abstract
What-aboutism deflection is not a communication failure. It is colonial technology - an automated institutional defence that activates when First Nations Peoples name specific harm and demand specific accountability. This piece argues that what-aboutism functions as a discursive mechanism with identifiable patterns, a documented history, and measurable consequences: in the 18 months following the Voice to Parliament referendum, over half of Aboriginal and Torres Strait Islander adults experienced discrimination when seeking healthcare. Discrimination is escalating - not improving - precisely as the frameworks designed to address it are being diluted.Drawing on Daniels’ structural harm frameworks, the documented co-optation of Dr Irihapeti Ramsden’s cultural safety into a universal one, and current Mayi Kuwayu data, this piece maps five patterns of what-aboutism, traces their institutional logic, and provides eight sovereignty-based responses for First Nations Peoples who choose to engage them. It closes with a direct address to the institutions and individuals producing the deflections it names.On January 26th, a white supremacist threw an explosive device into a crowd of Aboriginal and Torres Strait Islander Peoples in Perth, marching to change the date of Australia Day – “the anniversary of invasion, dispossession, and the beginning of policies that sought to erase us (Murray, 2026).”
A week and a half passed before authorities called it terrorism. The perpetrator remained unnamed "for his safety” - what Mununjahli and South Sea Islander Prof Chelsea Watego (2017) identified eight years earlier as “the privilege of white murderers of Black children: protection through anonymity while victims remain unknown.” Only after sustained pressure from Indigenous communities was the terrorist identified as Liam Alexander Hall (Torre, 2026).
The Bondi terrorists (Doherty et al., 2025) - brown men - were named within hours.
The responses that followed were predictable and cutting:
— "What about other communities?"
— "The bomb should have gone off."
— "He's a one off - he's been radicalised."
— "Who cares?"
Race determined who got called a terrorist immediately and who didn't. Race determined who received institutional protection and who was exposed. Race determined whose lives were grievable.
If you are an Indigenous person and you have ever raised specific harm against your communities only to have someone immediately redirect to other issues, other groups, other concerns - you know this pattern.
It has a name: "what-aboutism" deflection, or as I colloquially call it, the Shannon Noll effect (for non-Australians, this references a singer who famously covered the ‘Moving Pictures’ song "What About Me?"). And it's not random. It's colonial technology operating with precision to prevent the specific accountability you are demanding.
This guide gives you the tools to recognise it, understand what is actually happening, and respond from a place of sovereignty.
Defining What-Aboutism Deflection
DEFINITION
What-aboutism deflection is a discursive weapon that derails specific accountability by redirecting attention elsewhere. It operates as colonial technology: an automated defence system that activates when First Nations Peoples name specific harms and demand specific solutions.
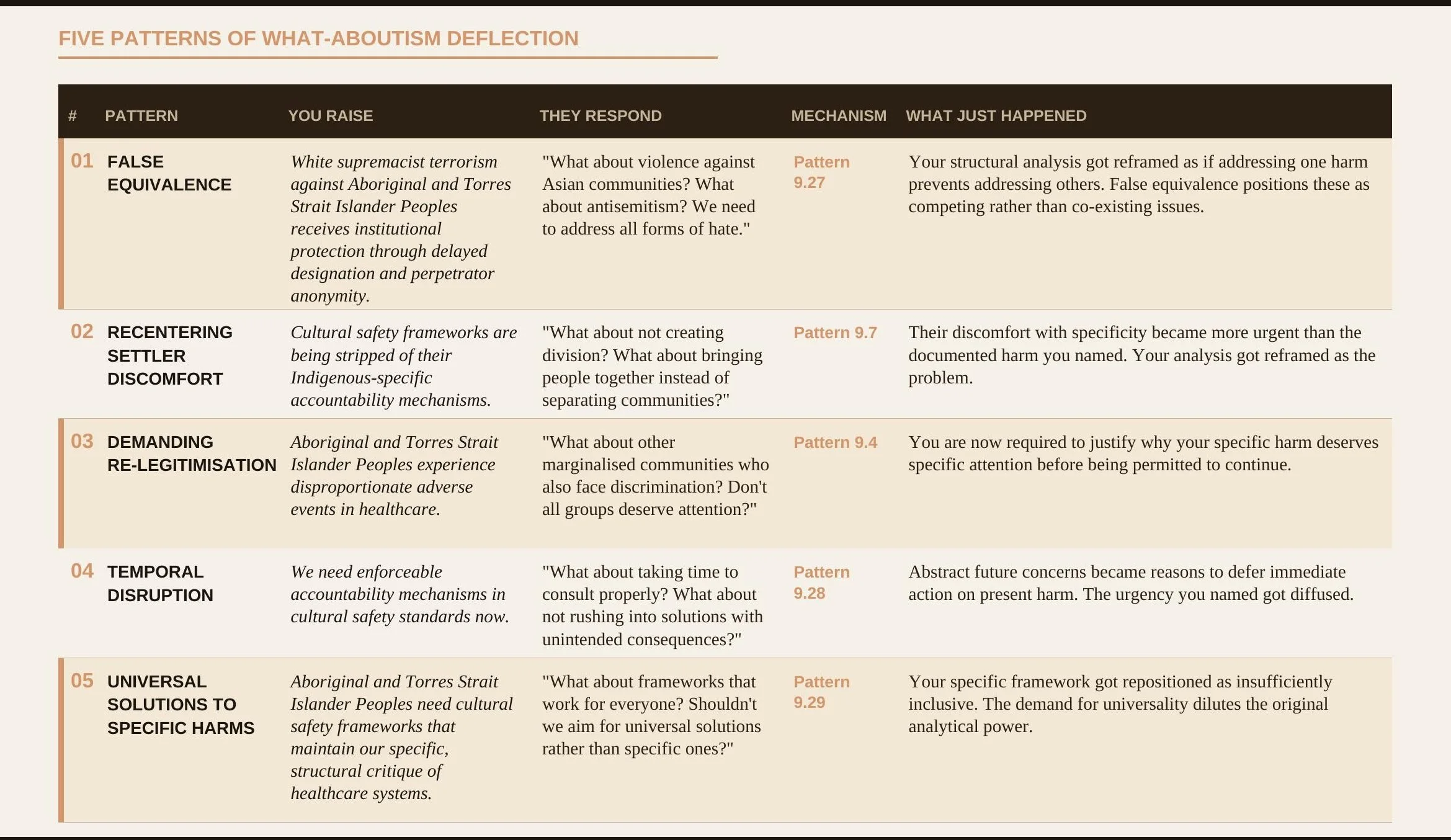
How It Operates
—False equivalence - positioning unrelated harms as competing priorities
— Recentering settler discomfort - making institutional unease more urgent than documented harm
—Demanding re-legitimisation - requiring Indigenous peoples to prove why Indigenous-specific solutions aren't exclusionary
— Temporal disruption - deferring action through concerns about process
— Universal dilution - insisting Indigenous frameworks must apply "to everyone" or they're unfair
What It Achieves
DEPLETION OF ORGANISING CAPACITY
Energy spent re-explaining is energy not spent organising for change.
DEFERRAL
Accountability is perpetually delayed pending "broader consultation."
DILUTION
Indigenous frameworks lose their sovereignty-based power analysis and are repositioned as one consideration among many.
MANUFACTURED ACTIVITY WITHOUT ACCOUNTABILITY
What-aboutism doesn't just exhaust and defer - it generates the appearance of institutional rigour. As Daniels (2025) observes, "recommendations have become a routine way for the [institution] to perform change without undergoing it" (p. 8). What-aboutism is how colonial institutions stay busy without ever having to change.
WHAT IT IS NOT
Genuine questions about implementation, coalition-building dialogue, or good-faith engagement with complexity. The distinction lies in intent and effect: genuine engagement seeks to understand Indigenous frameworks and build upon their structural rigour; what-aboutism deflection seeks to diffuse specificity, defer accountability, and protect white possessive investments in institutions.
This pattern is not random. This is not individuals being thoughtless. This is colonial technology functioning exactly as designed.
This pattern is not random. This is not individuals being thoughtless. This is colonial technology functioning exactly as designed.
How to Recognise What-Aboutism Deflection
Five predominant patterns, each mapped to the institutional mechanisms identified by Dr Shereen Daniels in 30 Patterns of Harm A Structural Review of Systemic Racism within the London Metropolitan Police Service (2025).
What's Actually Happening: The Theory
Scarcity Mindset
Safety is not scarce. Addressing Aboriginal and Torres Strait Islander Peoples’ disproportionate harm in healthcare does not prevent addressing other communities’ needs - it establishes the structural rigour required for everyone.
“For institutional racism to thrive, people need only be "colour blind," "meritocratic," ignore the reality of existing privilege and injustices, and simply let the systems and structures reproduce the status quo.”
- Elias & Paradies (2021, p. 47)
Daniels (2022) names the absurdity of this logic from her own experience of cancer treatment: no other consultant barged into her specialist’s office demanding he turn his attention elsewhere, no nurse complained her tests caused a backlog, and no cardiologist asked “What about my patients?” As she concludes: “Racism needs specific intervention. Taking a generalised approach to specific problems never yields impressive results” (pp. 156-157). The scarcity framing isn’t a reasonable concern about resource allocation. It is a mechanism for protecting institutional comfort at the expense of accountability.
Colonial Reflex
What-aboutism is how colonial powers protect themselves when threatened. When First Nations Peoples name specific harm and demand specific accountability, we threaten institutional arrangements that have never had to centre us. The reflex is automated colonial defence: diffuse our specificity, redirect attention away from structural critique, reframe our analysis as the problem, and exhaust us before we can organise for change.
White Possessiveness As A Foundation
Goenpul scholar Distinguished Professor Aileen Moreton-Robinson names the mechanism beneath this reflex: white possessiveness (2015). She argues that white possession operates at both ontological and epistemological levels. At the ontological level, "to be able to assert 'this is mine' requires a subject to internalise the idea that one has proprietary rights that are part of normative behaviour, rules of interaction, and social engagement" (Moreton-Robinson, 2015, p. 50).
“White possession operates discursively through narratives of the home of the brave and the land of the free… Against this stands the Indigenous sense of belonging, home, and place in its sovereign incommensurable difference.” - Moreton-Robinson (2015, p. 52)
The Co-optation of Cultural Safety: A Documented History
Cultural safety was developed by Ngāi Tahu, Rangitāne nurse Dr Irihapeti Ramsden as a structural critique. It centred Indigenous Peoples' authority to determine what constitutes safety in systems designed to harm us. It demanded institutions examine their own power, not just train practitioners in cultural awareness.
“Cultural safety was developed in the 1980s and 1990s as an Indigenous-led anti-colonial critique of nursing's Anglo-European knowledge base. It represented a bicultural, liberatory framework based on Te Tiriti o Waitangi and the notion of negotiated partnership between Māori as Tangata Whenua (people of the land) and settlers.” - Nurse academic, Dr Ruth De Souza (2026)
Australia now faces the same risk Aotearoa experienced in the 1990s and 2000s. There is growing pressure to broaden cultural safety frameworks beyond their Indigenous-specific foundations. While antisemitism is real and requires action, the solution is not appropriating Indigenous frameworks and stripping them of their sovereignty-based power analysis.
The contradiction is stark: the same Australian institutions resisting Aboriginal and Torres Strait Islander sovereignty claims have no difficulty supporting Zionist settler-colonial projects in Palestine. Apparently, Indigenous sovereignty is divisive when it's ours, but worthy of institutional investment when it's Israel's. This selective application reveals that what-aboutism is not about genuine solidarity - it's about protecting white possession by co-opting our frameworks while funding the dispossession of other Indigenous Peoples.
The colony does not abandon a framework it cannot immediately defeat. It waits. It asks reasonable questions. It broadens, dilutes, and repositions - until the framework that was built to hold it accountable becomes a tool it can use to protect itself. That is what De Souza (2026) documents in Aotearoa. That is what I witnessed across years of regulatory work in Australia. And that is what will happen here if we become complacent.
My parents’ and grandparents’ generation were denied access to culturally safe healthcare. They experienced racism seeking care, and they died in preventable ways because no accountability structure compelled anyone to do otherwise. What the National Law now contains - the principle that Aboriginal and Torres Strait Islander Peoples alone determine what is and isn’t culturally safe - is the structural answer to that. It took collective effort, sustained resistance, and years of fighting the same fight over and over to put it there.
Definition of Cultural Safety (National Law, Australia)
Cultural safety is determined by Aboriginal and Torres Strait Islander individuals, families and communities.
Culturally safe practise is the ongoing critical reflection of health practitioner knowledge, skills, attitudes, practising behaviours and power differentials in delivering safe, accessible and responsive healthcare free of racism. (Australian Health Practitioner Regulation Agency, 2020, p. 9)
We cannot rest on that victory. The definition must be actively defended - in every code review, every standard update, every conversation where someone asks why it can’t apply to everyone. Because the answer to that question is not a bureaucratic technicality. It is sovereignty. And sovereignty, in this country, has never been given. It has only ever been held.
The Documented Timeline of How Cultural Safety Was Stolen
1980s
Dr Irihapeti Ramsden (Ngāi Tahu, Rangitāne) develops Kawa Whakaruruhau ("cultural safety") as Māori-specific structural critique grounded in Te Tiriti o Waitangi. Core principles: Māori authority to determine safety; critical self-reflection by practitioners on their own power; structural transformation, not individual competency checklists.
1992
Nursing Council of New Zealand formally adopts Kawa Whakaruruhau into nursing and midwifery education.
1995
Parliamentary Select Committee investigation triggered by dominant group backlash.
1996
First broadening following external review: "The concept of cultural safety was then developed into a separate and broader philosophical perspective to change its primary focus from Māori and Kawa Whakaruruhau to the inclusion of all minority groups."
2002
Guidelines go further, separating cultural safety entirely from Te Tiriti and Māori health - what De Souza calls "a deflection and deferral of Indigenous sovereignty claims… conflating racialisation and colonisation."
2018
Ahpra introduces cultural safety into nursing and midwifery codes of conduct, 39 years after its development in Aotearoa, in a diluted form (Nursing and Midwifery Board of Australia, 2018).
2019
Ahpra releases its definition of cultural safety following a public consultation process (Ahpra, 2019), and was rightfully determined by Aboriginal and Torres Strait Islander health leaders.
2025
Curtis and colleagues publish refined definitions acknowledging the need to explicitly name power as central to cultural safety - what had been implicit in Ramsden's work but lost in translation (Curtis et al., 2025). The Nursing and Midwifery Board of Australia changed its definition to align with the National Scheme’s definition.
What De Souza's analysis reveals is not just that the framework was diluted. A specific, load-bearing element was removed. The 2002 broadening “didn't demolish the building - it left the paintwork standing and took out the steel frame” (Daniels, 2025, p. 12). You can mandate cultural safety training without ever centring Indigenous authority. You can claim progress while the harm escalates. As Daniels puts it: "Change the décor, and nothing shifts. Change the structure, and everything does" (2025, pp. 12-13).
THE POWER THAT WENT MISSING
“Cultural safety needs to explicitly focus on power… cultural safety foregrounds power differentials within society, the requirement for health professionals to reflect on interpersonal power differences, and how the transfer of power within multiple contexts can facilitate appropriate care.” - (Papps & Ramsden, 1996, p. 493)
WHEN DOMINANT GROUPS CLAIM "CULTURAL SAFETY"
De Souza (2026) names what happens when the framework gets inverted: "When a subject from a dominant group claims a need for cultural safety, even on behalf of another, they are also working against the idea that marginalised groups have specific knowledge that allows them to identify what is culturally safe. It is a discourse that erases and appropriates the affective space of marginality."
As De Souza concludes, cultural safety's transformation from a structural intervention to a tool of dominant groups now functions as "a form of gaslighting."
The Evidence: Discrimination Is Escalating, Not Improving
Data from Mayi Kuwayu: The national study of Aboriginal and Torres Strait Islander wellbeing shows that in the 18 months since the Voice to Parliament referendum (October 2023 - April 2025), over half (51.8%) of Aboriginal and Torres Strait Islander adults experienced discrimination when seeking healthcare. Vicarious racism - hearing jokes, insulting comments, or witnessing unfair treatment - is pervasive at 78.8% (Wilkes et al., 2025).
This is not improvement. This is escalation. And it's happening precisely as cultural safety frameworks get diluted into universal approaches that avoid naming racism and avoid the explicit power analysis Ramsden embedded from the beginning.
The data does not capture the full picture. Aboriginal and Torres Strait Islander health professionals experience racism frequently at work, and often face resistance or retribution when they identify injustices (Fuller et al., 2024; Wilkes et al., 2026). This is the structural function what-aboutism serves in practice environments - it does not simply deflect patients’ experiences of racism. It suppresses the capacity of the very practitioners most equipped to name and challenge it. What-aboutism is not just a conversation tactic. It is a workforce mechanism.
Yet data alone does not move institutions. Daniels (2022) is precise about why: "data is also an output. It measures things after the fact. It measures the what, not the why" (p. 180). The Mayi Kuwayu figures tell us what is happening to Aboriginal and Torres Strait Islander Peoples in healthcare. They do not tell us why institutions that have seen this data for years remain unmoved by it. What-aboutism is part of the answer - it provides the mechanism by which institutions acknowledge the what while perpetually deferring the why.
Bond, Whop, Singh and Kajlich (Bond et al., 2020) name this pattern with precision - Bond (writing as Watego) among them. The statistical story of Indigenous health and death has been reported in federal parliament for over a decade - an annual account-keeping exercise of policy failure that never translates to improved outcomes. The contrast they draw is instructive: when COVID-19 threatened, institutional action was swift. The ongoing pandemic of racism that Indigenous Peoples have been fighting since 1788 produced no equivalent mobilisation. This is not institutional incapacity. It is institutional indifference - and indifference is a structural choice, not an oversight.
Why Exhaustion Is the Point
Every what-aboutism requires you to re-explain why your specific issue matters; re-establish your legitimacy to centre it; re-justify why addressing it specifically isn't exclusionary; and defend against the implication you don't care about other communities.
That exhaustion is not a side effect. It's the design. Colonial systems have avoided accountability for centuries, not through outright refusal alone, but through infinite deferral - always another perspective to balance, another community to consider, another reason now is not the moment.
Sovereignty-Based Responses: What You Can Do
You are not obligated to engage every deflection. Your energy has value. Protect it. But when you choose to respond, here are frameworks grounded in sovereignty.

For Non-Indigenous People Reading This
When you respond to First Nations Peoples' specific analysis with what-aboutism, you are reasserting your authority to determine what gets discussed; protecting institutional comfort at the expense of accountability; positioning your discomfort as more urgent than documented harm; and performing thoughtfulness while preventing change. This is not allyship. This is colonial power protecting itself through your body.
Why You Do It
Scarcity Mindset
The scarcity logic examined earlier is worth naming directly here. You genuinely believe addressing Indigenous-specific harm takes something away from others. This is factually wrong - and it reveals you have never had to operate in systems that were not designed for you. When you have always been centred, specificity reads as exclusion.
White Acceptance As Structural Checkpoint
As Daniels names it: "white acceptance becomes the gateway to recognising and addressing racial harm" (2025, p. 6). When you ask, "What about other communities?" you are not being thorough. You are operating as a checkpoint, requiring First Nations Peoples to obtain your acceptance before their analysis can proceed. That is colonial power with good intentions, which produces the same outcomes as colonial power without them.
"Colour Blind" Institutional Racism
As Elias and Paradies show, "for institutional racism to thrive, people need only be 'colour blind,' 'meritocratic,' ignore the reality of existing privilege and injustices, and simply let the systems and structures reproduce the status quo" (2021, p. 47). Your neutrality is the problem.
White Possessiveness
As Moreton-Robinson (2015) explains, you've internalised proprietary rights over institutions and their frameworks. When First Nations Peoples assert sovereignty claims, it threatens that unconscious assumption.
Automated Colonial Reflex
You're doing what colonial systems trained you to do - diffuse, defer, dilute. This doesn't make you a bad person. It makes you someone operating from unexamined defaults.
What To Do Instead
— Sit with the discomfort of not being centred. When First Nations Peoples centre their own analysis, your job is to listen. Not balance. Not broaden. Listen.
— Recognise that specificity enables coalition. Coalition requires specificity, not false universality.
— Understand the history you’re erasing. De Souza (2026) documents the 2002 broadening as a deliberate deferral of Indigenous sovereignty claims. When you expand frameworks without maintaining our safety as paramount, you’re participating in documented theft.
— Acknowledge racism is escalating - the data is there. This happened while institutions were being “thoughtful” about avoiding the division of communities.
— When you notice the what-aboutism impulse, stop. Ask yourself: "Does this demonstrate engagement with what was actually said, or am I changing the subject?" If it's the latter - don't say it.
Your Authority Is Not In Question
For First Nations Peoples reading this: every time you experience whataboutism deflection, you are experiencing a sovereignty violation. Someone is asserting their authority to determine whether your analysis deserves specific attention.
Your authority is not in question. You do not need their permission to centre your community's safety.
When cultural safety gets co-opted, diluted, or universalised without Indigenous Peoples' authority determining what safety requires, that is theft. When the explicit power analysis gets removed, that is disarming. When it gets inverted so dominant groups claim they need "cultural safety" from your critique, that is gaslighting. When you're told your specific needs must be "balanced" against others, that is colonial logic encoded as equity.
That refusal - refusing to re-legitimise, refusing to justify, refusing to exhaust yourself proving what you already know - is sovereignty in action.
A Final Word to Institutions
The question facing institutions, regulators, and settler communities is not whether they agree with this analysis. They have read it. They have sat in the rooms where these deflections were deployed. They have watched the data accumulate and the frameworks dilute. The question is whether they will become the next exhibit in the next version of this article - or whether they will do the structural work their stated commitments require.
That work has a specific shape. It is not a workshop. It is not a policy commitment. It is the active, enforceable refusal to produce the deflections this article names - in every code review, every standard update, every room where someone asks why we can’t broaden the definition. The deflection has a name now. Using it is a choice.
Reference List
Ahpra. (2019). Ahpra Consultation Report on Cultural Safety Definition [Public Consultation]. Australian Health Practitioner Regulation Agency. https://www.ahpra.gov.au/documents/default.aspx?record=WD20%2f29578&dbid=AP&chksum=WNtpskiQJ01zHJQqObbIow%3d%3d
Australian Health Practitioner Regulation Agency. (2020). National Scheme’s Aboriginal and Torres Strait Islander Health and Cultural Safety Strategy 2020-2025. Australian Health Practitioner Regulation Agency. https://www.ahpra.gov.au/documents/default.aspx?record=WD20%2f29563&dbid=AP&chksum=7v438b3dSNNx%2bd9zleWRbA%3d%3d
Bond, C. J., Whop, L. J., Singh, D., & Kajlich, H. (2020). “Now we say Black Lives Matter but … the fact of the matter is, we just Black matter to them”1. Medical Journal of Australia, 213(6). https://www.mja.com.au/journal/2020/213/6/now-we-say-black-lives-matter-fact-matter-we-just-black-matter-them1
Curtis, E., Loring, B., Jones, R., Tipene-Leach, D., Walker, C., Paine, S.-J., & Reid, P. (2025). Refining the definitions of cultural safety, cultural competency and Indigenous health: Lessons from Aotearoa New Zealand. International Journal for Equity in Health, 24(1), 130. https://doi.org/10.1186/s12939-025-02478-3
Daniels, S. (2025). A Structural Companion Guide: For 30 Patterns of Harm: A Structural Review of Systemic Racism within the London Metropolitan Police Service. London Metropolitan Police Service. https://www.met.police.uk/SysSiteAssets/media/downloads/force-content/met/about-us/london-race-action-plan/a-structural-companion-guide.pdf
De Souza, R. (2026). On the misuse of Cultural Safety. Overland Literary Journal, 259(Feb/March 2026). https://overland.org.au/2026/02/on-the-misuse-of-cultural-safety/
Doherty, B., Evershed, N., & Shimada, Y. (2025, December 15). Visual explainer: How a night of terror unfolded in Bondi. The Guardian. https://www.theguardian.com/australia-news/2025/dec/15/a-visual-guide-to-the-bondi-beach-terror-attack
Fuller, J., Browning, M., Evans, J., & Balvin, N. (2024). How To Attract, Retain and Grow the Aboriginal and Torres Strait Islander Health Workforce in Australia: A self-determined approach: - ACHSM Asia-Pacific Health Leadership Congress in Brisbane 2024. Asia Pacific Journal of Health Management, 19(3), Article 3. https://doi.org/10.24083/apjhm.v19i3.4163
Moreton-Robinson, A. (2015). The white possessive: Property, power, and Indigenous sovereignty. University of Minnesota Press.
Murray, N. (2026, January 26). The question is no longer why the date should change, it is whether Australia has the courage to begin the next chapter in our nation’s story. National Indigenous Times. https://nit.com.au/26-01-2026/22302/the-question-is-no-longer-why-the-date-should-change-it-is-whether-australia-has-the-courage-to-begin-the-next-chapter-in-our-nations-story
Nursing and Midwifery Board of Australia. (2018, March 1). New codes of conduct take effect for nurses and midwives. https://www.nursingmidwiferyboard.gov.au/News/2018-03-01-new-codes.aspx
Papps, E., & Ramsden, I. (1996). Cultural Safety in Nursing: The New Zealand Experience. International Journal for Quality in Health Care, 8(5), 491–497. JSTOR.
Torre, G. (2026, February 17). Invasion Day bombing suspect named as suppression order deemed “not in the interests of justice.” National Indigenous Times. https://nit.com.au/17-02-2026/22718/invasion-day-bombing-suspect-named-as-suppression-order-deemed-not-in-the-interests-of-justice-alleged-terrorism
Watego, C. (2017, October 16). We just Black matter: Australia’s indifference to Aboriginal lives and land. The Conversation. https://doi.org/10.64628/AA.7js4rxn6t
Wilkes, B., Colonna, E., & McKay, C. (2025). Monitoring Aboriginal and Torres Strait Islander mental health and wellbeing around the Voice to Parliament Referendum. Yardhura Walani, ANU. https://yardhurawalani.com.au/wp-content/uploads/2025/12/Report_Tracking-wellbeing-18-months-post-Referendum.pdf
Wilkes, B., Whop, L., Thurber, K., Colonna, E., & Lovett, R. (2026). Embedding cultural safety to combat racism against Aboriginal and Torres Strait Islander peoples: Advice for healthcare settings. Australian Journal of General Practice, 55, 91–96.
Jayde Fuller is a Gamilaraay woman operating from Quandamooka Country. She is the founder of Indigenous Regulatory Practice and spent seven years in health practitioner regulation, including leading the work that embedded self-determination into the definition of cultural safety used across sixteen health professions in Australia's National Law. This article is an output of that practice.